Hussein Ageely1,
Ibrahim Bani2,
Abdelrahim Gaffar3,
Magdeldin Eltigani4,
Abu Obaida Yassin1,
Badria Said5,
Mohamed Salih Mahfouz3 ![]()
For correspondence:- Mohamed Mahfouz Email: mm.mahfouz@gmail.com
Received: 15 June 2015 Accepted: 29 December 2015 Published: 29 January 2016
Citation: Ageely H, Bani I, Gaffar A, Eltigani M, Yassin AO, Said B, et al. Prevalence and risk factors for brucellosis in Jazan Province, Saudi Arabia. Trop J Pharm Res 2016; 15(1):189-194 doi: 10.4314/tjpr.v15i1.26
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose:Brucellosis is responsible for considerable public health issues involving economic losses due to abortion, loss of milk production and infertility in adult males. The purpose of this study was todetermine the sero-prevalence of brucellosis in Jazan Province, Saudi Arabia and assess the possible risk factors.
Methods:An observational cross-sectional study was conducted in three geographical areas of Jazan Province, Saudi Arabia. The study sample included 400 participants from randomly selected primary health care centres. A standardised questionnaire was used to collect information on demographics and risk factors for brucellosis. A 5 ml blood sample was collected from each study participant. The SPSS statistical program was utilised for data analysis.
Results:The overall sero-prevalence of brucellosis in Jazan Province was 13.4 % and was higher among participants ≥ 40 years old (20 %) than those < 40 years (12 %). Prevalence was significantly higher among rural (39.3 %; 95 % confidence interval [CI], 29.8 – 49.7) than urban populations (4.6 %; 95 % CI, 2.7 – 7.9), in Saudis (14.5 %; 95 % CI, 11.1 – 18.8) than non-Saudis (3.0 %; 95 % CI, 7.0 – 15.3) and in males (16.4 %; 95 % CI, 12.2 – 21.6) than females (7.1 %; 95 % CI, 3.7 – 13.4).
Conclusion:These results indicate the need for a vaccination program in Jazan Province and for public awareness campaign activities to combat and eradicate the disease.
Introduction
Brucellosis is a major zoonotic infection that remains an important public health concern in many parts of the world [1]. In addition to its impact on human health, brucellosis is responsible for considerable public health issues involving economic losses due to abortion, loss of milk production and infertility in adult males [2].
Four important species are pathogenic to humans, such as Brucella melitensis, found primarily in goats, sheep and camels, Brucella abortus in cows, Brucella suis in pigs and Brucella canis in dogs. Brucella spp. differ in their degree of virulence and invasiveness. B. melitensis is the most invasive and results in the most severe illness. B. abortus is the least invasive and causes the mildest illness. B. melitensis remains the principal cause of human brucellosis worldwide [3,4].
Brucellosis has a worldwide distribution, but the disease has become rare among most industrialised countries because of routine domestic livestock screening, implementation of effective animal vaccination programs and strict regulations regarding animal importation and other precautionary measures. However, brucellosis remains leading zoonoses in developing countries of the Eastern Mediterranean, including Saudi Arabia [4-6].
Human brucellosis ranks as the number one priority zoonosis among Member States of the Eastern Mediterranean including Saudi Arabia [8,9]. In 1999, the World Health Organisation (and Food and Agriculture Organisation Report on Brucellosis) revealed Saudi Arabia to have the highest incidence of human brucellosis in the province [10]. Literature from Saudi Arabia suggests that B. melitensis remains the principal cause of human brucellosis, with less frequent infections by B. abortus. Furthermore, the natural reservoir for brucellosis is domestic animals, and animal-to-animal transmission is usually venereal or via ingestion of infected tissues or milk [11-14].
Although sero-prevalence data on brucellosis are not available for most provinces in Saudi Arabia [4,5,11,14], no study has assessed the disease in Jazan Province, southwest Saudi Arabia. The aim of this study was to obtain an estimate of the prevalence of human brucellosis in Jazan Province and to identify possible associated risk factors among the people living in this province.
Methods
Study design and setting
An observational cross-sectional survey was conducted in three geographical areas of Jazan Province. Jazan (also called Gizan) is one of the 13 provinces of the Kingdom of Saudi Arabia. It is located on the tropical Red Sea coast in southwestern Saudi Arabia.
Participants and sampling procedures
A sample size of 400 participants (≥ 15 years old) who attended selected primary heath care centres (PHCCs) and signed informed consent were included in the study. The provinces were divided into mountain, coastal and plain areas for sampling purposes. One province was chosen randomly from each area, and two PHCCs were selected. Probability proportional to the sample size was used to determine the number of participants used from each of the selected PHCCs. The study was conducted from May 2012 – March 2013.
Sample collection and laboratory processing
A 5 ml blood sample was collected from each individual, centrifuged to separate the serum and dispatched on the same day to the Faculty of Medicine Laboratory. Sera were stored at −70 °C for subsequent testing.
The Diagnostic Automation Brucella IgG antibody enzyme-linked immunosorbent assay test kit was used to detect specific IgG antibodies against Brucella in sera. Diluted sera (1:101) and ready-to-use standards were pipetted into the wells of a microtiter plate, and the IgG antibodies in the serum and the immobilised Brucella antigen were bound. After 1 h of incubation at room temperature, the plate was rinsed with diluted wash solution to remove unbound material. Then, the ready-to-use anti-human-IgG peroxidase conjugate was added and incubated for 30 min. After another wash, the substrate (TMB) solution was added and incubated for 20 min to develop a blue colour. Colour development was terminated by adding the provided stop solution, which changed the colour from blue to yellow. The resulting dye was measured at a wavelength of 450 nm using the ELx800 Microplate Reader (BioTek, Winooski, VT, USA) with Gen5 software for data output. The calculated absorption values were compared with the standard cut-off values. A sample was considered positive if its value was > +20 % of the standard cut-off value. Values below the standard cut-off were considered negative.
Data collection and study instrument
In addition to the blood samples, other demographic and risk factor data were collected through personal face-to-face interviews. A questionnaire was used to record age, sex, nationality, place of residence, consumption of raw milk (yes or no), consumption of camel’s milk (yes or no), consumption of cheese (yes or no), contact with a dead animal (yes or no), contact with animals (yes or no) and other risk factors.
Statistical analysis
The overall sero-prevalence of brucellosis among the study participants was calculated using 95 % confidence intervals (CI). The chi-square test or Fisher’s exact test was used to evaluate the sero-prevalence of brucellosis among the different sub-groups. Crude odds ratios (ORs) were obtained by univariate analysis to determine the association of each variable with brucellosis sero-prevalence. All statistical tests were two-sided; and a p < 0.05 was considered significant. The statistical analysis was performed using SPSS ver. 17.0 (SPSS Inc. Chicago, IL, USA) software.
Ethical considerations
Ethical approval for this study was obtained from the Ethics Committee of the Faculty of Medicine, Jazan University. Informed written consent was obtained from all participants prior to involvement in the study.
Results
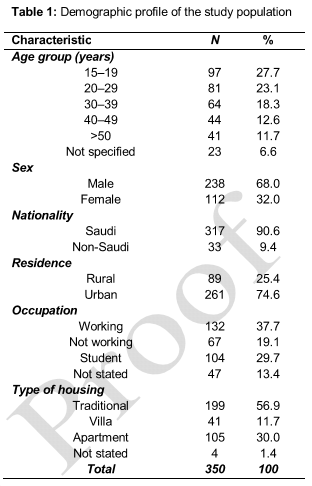
shows the demographic characteristics of the study population. A total of 350 participants provided signed consent and were included (response rate, 87.5 %). Almost 50 % of the subjects were < 30 years old; majority of them were Saudi (90 %) males (68 %) and were living in an urban area (74.6 %).
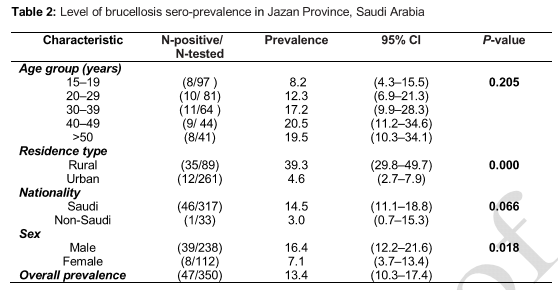
shows the brucellosis sero-prevalence level in Jazan Province. The overall sero-prevalence of brucellosis in Jazan Province was 13.4 % and higher among those > 40 years old. Prevalence was significantly higher among rural (39.3 %; 95 % CI, 29.8– 49.7) versus urban (4.6 %; 95 % CI, 2.7–7.9) populations, Saudis (14.5 %; 95 % CI, 11.1–18.8) versus non-Saudis (3.0 %; 95 % CI, 0.7–15.3) and males (16.4 %; 95 % CI, 12.2–21.6) versus females (7.1 %; 95 % CI, 3.7– 13.4).
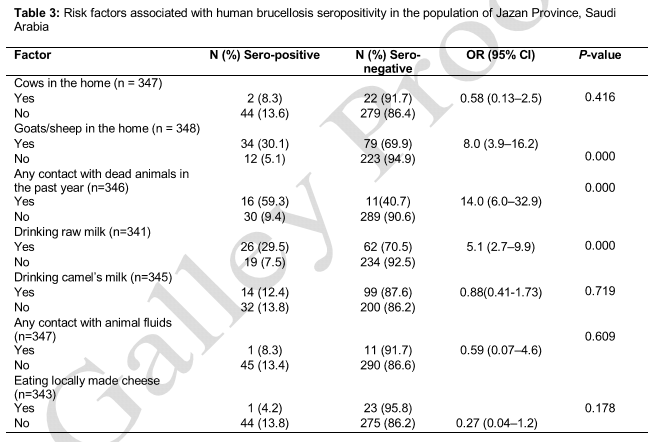
shows the association between certain factors and brucellosis seropositivity in the Jazan Province population. Seropositivity was significantly associated with keeping goats/sheep in the home, contact with dead animals in the past year and drinking raw milk. No significant association was found between seropositivity and keeping cows in the home, drinking camel’s milk, contact with animal fluids or eating locally made cheese.
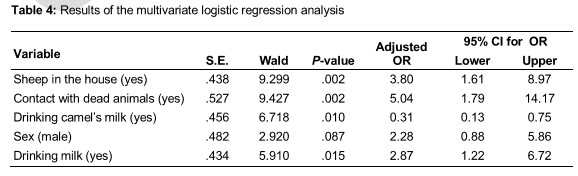
illustrates the results of the multivariate logistic regression analysis. The analysis showed that seropositivity was significantly association with contact with dead animals in the past year (OR, 5.04; p = 0.002), keeping goats/sheep in the home (OR, 3.80; p = 0.002), drinking raw milk (OR, 2.87; p = 0.015) and drinking camel’s milk (OR, 0.31; p = 0.010).
Discussion
This is the first study to examine the sero-prevalence of and risk factors for human brucellosis in Jazan Province, Saudi Arabia. The results revealed that the overall sero-prevalence of brucellosis in Jazan Province was 13.4 %, which was higher among those > 40 years old. Prevalence was higher among males (16.4 %) than females (7.1 %), which was a similar finding in many studies in Saudi Arabia and other Arabian countries [15-17]. The higher rate of brucellosis sero-prevalence in males compared with females was probably due to a greater involvement of men in domestic animal farming and product handling. The overall prevalence was similar to that in other studies conducted in Saudi Arabia [17].
We found a higher sero-prevalence rate in rural areas (39.3 %), which was higher than that reported in other parts of Saudi Arabia (26.2 %) [18]. The variation in the prevalence rates of brucellosis among different geographical regions may be due to variations in disease prevalence among animals, occupational contact or the social habits of different populations. The sero-prevalence of brucellosis was found to increase with age, which is consistent with observations made in Iran, Jordan, Lebanon and Kuwait [19,20]. The lower sero-prevalence rates found in teenagers, compared with adults, may be due to greater exposure of adults to livestock.
A major risk factor, seen in 5.9 % of sero-positive cases, was contact with dead animals. Brucellosis sero-positivity was significantly associated with keeping goats/sheep in the house, contact with dead animals during the past year and drinking any kind of raw milk. These findings agree with those of other studies [8]. Drinking camel’s milk is a common practice and custom in Saudi Arabia, but it had no association with brucellosis sero-positivity.
Limitations of the study
Although the present study is the first to consider brucellosis in Jazan Province, it has some significant limitations. First, the study was based on a relatively small sample size, so the brucellosis prevalence results should be interpreted carefully. Second, our participants were patients attending Jazan Province PHCCs and thus may not truly represent the Jazani population. Finally, this was a cross-sectional study design, which is not suitable for assessing brucellosis risk factors, as direct and causal relationships among the variables cannot be established properly.
Conclusion
This study confirmed the risk of brucellosis in Jazan Province. The current results confirm the need for a vaccination program and a public awareness campaign to limit and eradicate the disease. We strongly recommend the development of methods to detect brucellosis, initiate early treatment and reduce complications.
Declarations
Acknowledgement
References
Archives


News Updates